Going for the Distal Radial Artery : Tips & Pearls
A. Fauzi Yahya
Department of Cardiology and Vascular Medicine Padjadjaran University/Hasan Sadikin General Hospital
Bandung-Indonesia
Distal transradial access (dTRA) in the anatomical snuffbox is a newly emerging approach for cardiac intervention and has gained increasing popularity among interventional cardiologist.
This novel approach can overcome some drawbacks of standard radial artery cannulation in several aspects.
History
Drs Avtandil Babunashvili and Alexandr Kaledin from Russia were the first to introduce the concept of dTRA. Dr Babunashvili initially used distal access for recanalization of occluded ipsilateral radial arteries in a retrograde way (1). Dr Kaledin presented data in 2014 at the EuroPCR meeting on a large group of patients who had undergone distal radial access. Both operators influenced Dr Farshad Roghani-Dehkordi from Iran to attempt distal access himself because many of his female patients wear bracelets that cover the forearm. Dr Roghani presented a series of patients undergoing distal radial access at the Third Isfahan Transradial Course in Iran in 2016, where Dr Kiemeneij was also lecturing (2,3). Dr Kiemeneij first reported left dTRA in the anatomical snuffbox for interventional therapy in 2017 (2). Shortly after his published paper, several large studies were performed to evaluate the safety and feasibility of this new approach. This novel approach was rapidly disseminated via Twitter and other social media unlike through traditional in-persons meeting or publications.
Anatomical Point of View
The radial artery descends along the lateral side of the forearm above the radius towards the wrist, where it is palpable between the tendon of the flexor carpi radialis medially and the anterior border of the radius where the conventional transradial access (TRA) is. At the wrist, the radial artery gives rise to the superficial palmar branch, which passes through the thenar muscles, and anastomose with the end of the ulnar artery to form the superficial palmar arch. Distally, the radial artery curls postero-laterally to pass onto the dorsal aspect of the wrist (4). The radial artery then anastomoses with the deep branch of the ulnar artery to complete the deep palmar arch. Sometimes the superficial and deep palmar arch are incomplete or undeveloped.
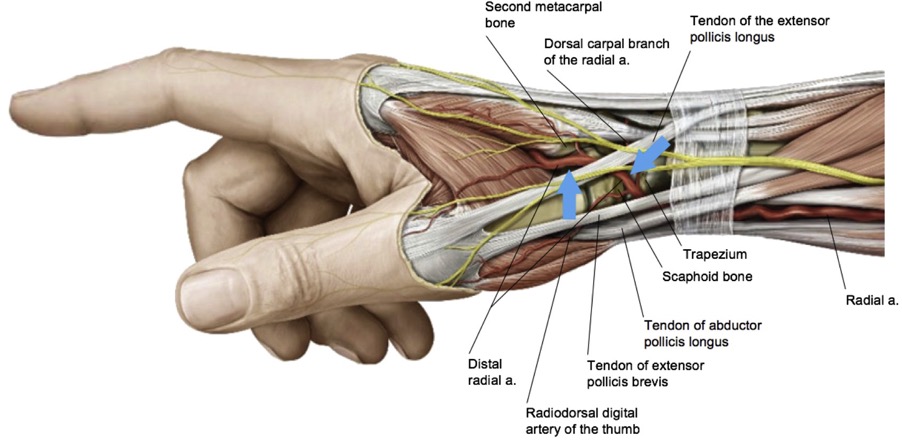
There are 2 sites where the pulse of radial artery in the dorsum of hand can be felt (Image 1). The first is the anatomical snuffbox which is a triangular depression space on the radial, dorsal aspect of the hand, showing up when the thumb is extended.
The snuffbox has three borders, floor and roof. The medial border is the tendon of extensor pollicis longus muscle. It is surrounded laterally by the tendons of abductor pollicis longus and extensor pollicis brevis muscles. Proximal border is styloid process of the radius.
The anatomical snuffbox has a “bone basement” composed of distal radius, scaphoid, trapezium and the base of the first metacarpal bone . The roof is formed by the skin and superficial fascia, in where we can find the cephalic vein and superficial branch of the radial nerve . Consequently, radial artery in this area is easily palpable and compressed to hemostasis.
Another available puncture site of distal radial artery is the first intermetacarpal space, precisely in the vertex of the angle between the long extensor and the second metacarpal
bone. As a continuity of the radial artery in the anatomical snuffbox, the radial artery in this area is superficial too (4,5).
Most researches have applied the distal approach at the anatomical snuffbox. The attempts in the first metacarpal space are rare, possibly because of the greater technical challenge and higher failure rate.
The Pearls
The distal radial approach is considered a further refinement of the standard routine radial access and provide an additional non-femoral access-site option. Patients with various orthopaedic limitations including frozen shoulders and elbows, who are unable to supinate their arm can benefit from this new arm position.
The dTRA snuffbox approach potentially can decrease the incidence of radial artery occlusion due to the two different arterial networks at the wrist, viz one superficial and another deep, connecting the radial with the ulnar artery in forming the palmar arch.
Other potential advantage of dTRA is the ability of the patient to mobilize their wrists with no increased risk for vascular complications given the direct pressure of the haemostatics band against the scaphoid bone. This approach can potentially reduce hemostasis duration. The proximal radial artery can be preserved for future procedures such as bypass grafting, or arterio-venous shunts.
There are also several additional advantages of using left distal radial access (ldTRA). These include improved operator’s comfort during the procedure (Image 2) and lower exposure to radiation, the ability to perform angiography in patients with prior CABG with LIMA graft. Right-handed patients do not need to be bothered by the restrained movement of right hand after catheterization.

Natural working position of the operator during performing PCI via left distal radial artery
Limitations
The limitations of distal left radial artery approach are similar to that of all radial artery access, which include radial artery tortuosity, anatomical variances, subclavian tortuosity precluding successful cannulation.
As with every new procedure, there is a learning curve for the dTRA approach. The puncture of the dTRA can be challenging and requires longer time due to its smaller diameter. Kim et al. reported that the average diameter of radial artery in anatomical snuffbox was 2.57mm in 101 Korean individuals, while it is 2.65mm at the wrist. Women have smaller diameter and higher failure puncture rate of distal radial artery than the man. (6) The small-calibred distal radial artery may limit the size of sheaths and catheters used. This may affect the success of high complex procedures. In selected patients, the use of 7 Fr sheath is feasible and safe (7).
Another problem is the length of catheters. Most catheters are designed for conventional puncture site at present, so these devices could be not long enough when the puncture site is about 5 cm blow the conventional site. The operators may have to perform coronary procedure “on the tip” of the catheter especially in taller patients.
A review of the most recent literature on distal radial access reveals relatively few reported procedure-related complications. Most reported are hand hematomas of varying degrees. Others include radial artery occlusion and dissection. We reported a case of pseudoaneurysm (PSA) in a patient who underwent coronary angiography via dTRA 3 months prior (8).
Puncture Technique
In the case of right distal radial access, the right upper arm is positioned in a semi-pronated manner. To access left distal radial artery, the left hand is bent over towards the patient’s right groin. After disinfection, the patient is covered with a sterile drape and asked to clasp his thumb under the other four fingers, with the hand slightly abducted. After disinfection and local anesthesia, the artery is punctured preferably with a 21 gauge (G) open needle, at an angle of 30-45 degrees in a lateral to medial direction. The needle is directed to the point of strongest pulse, proximally in the anatomical snuffbox. A through and- through puncture is not recommended, since the needle will touch the periosteum of the scaphoid or trapezium bones, which can be painful. Ultrasound guided puncture may be helpful to assess distal radial artery location.
After successful puncture, a flexible, soft, J-shaped 0.21” metallic wire is inserted. This is followed by a small skin incision and sheath insertion. As the dorsal skin of the hand is thicker than the palmar side, some operators suggest making a deeper skin incision and to insert the introducer first before introducing the whole assembly sheath (video 1). A spasmolytic cocktail consisting of 200 mcg of nitroglycerine and weight-based heparin is given after successful insertion of the sheath.

Puncture and sheath insertion
Hemostasis Management
The distal radial artery access has the potential to become the safest and most convenient access for coronary angiography and intervention, due to its location in the hand directly above the proximal and distal row of the carpal bones. The bone provides support when hemostatic compression is performed. In contrast, the proximal radial artery lies more parallel than perpendicular along the radius bone at the wrist. The distal radial artery access has the advantage over the femoral artery of providing a more effective hemostasis, since it is superficial, readily accessible by ultrasound, and about 4 times smaller in calibre than the femoral artery.
Patent hemostasis is recommended which means applying just enough pressure to prevent bleeding through the vascular puncture, but not so much as to cause complete collapse of the vessel under pressure resulting in flow cessation. There are several methods of hemostasis. These include applying elastic bandage with gauze roll, use of TR-Band or similar device, or band with air bladder. A dedicated hemostasis device for distal radial artery access is now available in the market which provides effective and comfortable compression (name?). Regardless, hemostasis in dRA is usually achieved within 3 hours. Patient can move his wrist even as hemostasis is being applied, which enhances the comfort level.
Conclusion
Mastering distal transradial access increases the access options for operators and improve the comfort level for patients. Current literature indicates that distal radial artery access is reliable, safe and effective. More data is required in a randomized controlled trial fashion to fully evaluate the advantage of this access compared to the proximal conventional right radial access.
References
- Babunashvili A, Dundua D. Recanalization and reuse of early occluded radial artery within 6 days after previous transradial diagnostic procedure. Catheter Cardiovasc Interv 2011; 77: 530-6
- Kiemeneij F, Klass D, Nathan S. Keep an open mind about distal radial access. Cath Lab Digest. 2019 Mar; 27(3)
- Kiemeneij F. Left distal transradial access in the anatomi¬cal snuffbox for coronary angiography (ldTRA) and inter¬ventions (ldTRI). EuroIntervention 2017; 13:851-857.
- Cerda A, del Sol M. Anatomical snuffbox and it clinical significance. A literature review. Int J Morphol 2015; 33: 1355-60.
- G. A. Sgueglia, A. Di Giorgio, A. Gaspardone, and A. Babunashvili, “Anatomic basis and physiological rationale of distal radial artery access for percutaneous coronary and endovascular procedures,” JACC: Cardiovascular Interventions 2018; 11: 2113–2119 2
- Y Kim, Y Ahn, MC Kim et al Gender differences in the distal radial artery diameter for the snuffbox approach. Cardiology Journal 2018; 25: 639–641
- Gasparini GL, Garbo R, Gagnor A, Oreglia J, Mazzarotto P. First prospective multicenter experience with left distal transradial approach for coronary chronic total occlusion interventions using a 7 Fr Glidesheath slender. EuroIntervention 2019; 15: 126-128
- Yahya AF Pramudyo M, Iqbal M, et al. Pseudoaneurysm After Left Distal Transradial Access. Cath Lab Digest 2019; 10 (27)