"Double Kissing String Culotte Technique" for bifurcation PCI: Could we make it real with modern generation of stent?
Yu-Ho Chan, Pok Oi Hospital, Hong Kong
Introduction
Bifurcation remains a challenge in percutaneous coronary intervention (PCI). Each bifurcation lesion is unique; therefore, each bifurcation lesion should be managed individually. Provisional stenting technique is generally recommended in most bifurcation lesions especially in non-true simple bifurcation lesion. On the other hand, for complex bifurcation lesions, 2-stent technique especially DK-Crush technique is recommended (1).
Each 2-stent bifurcation technique has its drawback in terms of multiple layers of overlapping, malapposition and stent distortion.
A novel 2-stent bifurcation technique - the Double Kissing String Culotte Technique, will be introduced in this article.
String-Culotte Technique/the Cross-Stent Technique
String-Culotte Technique was first described by Kawasaki et al in 2010. They named the technique as the Cross-Stent Technique. Generally, it is a modification of culotte technique (one to two stent strut protruding from the side branch into the main vessel). This technique aims at minimizing the overlapping of the stent struts in the 2-stent technique. (2)
Gabor G et al subsequently studied and renamed this technique as Single String-Culotte Technique in 2015. With the guidance of the Optical Coherence Tomography (OCT) using modern drug eluting stent, the technique was found to be feasible and safe. (3)
Procedural steps of Double-Kissing String Culotte Technique:
Procedural steps were illustrated by PCI to a bifurcation lesion at the left circumference (Lcx) and the obtuse marginal (OM).
(1)A stent was precisely positioned at the side branch with coverage of the superior edge of ostium, and minimal protrusion of one to two stent strut into the main branch (Fig 1).

Figure 1
The stent was post-dilated with non-compliance balloon. (2)A workhorse wire was buckled into the side branch. It was pulled back until it dropped into the protruded single stent cell in the main vessel. The wire was then advance distally in main branch. (3) Wire position was confirmed by OCT (Fig 2a-2b, online video 2a-b).
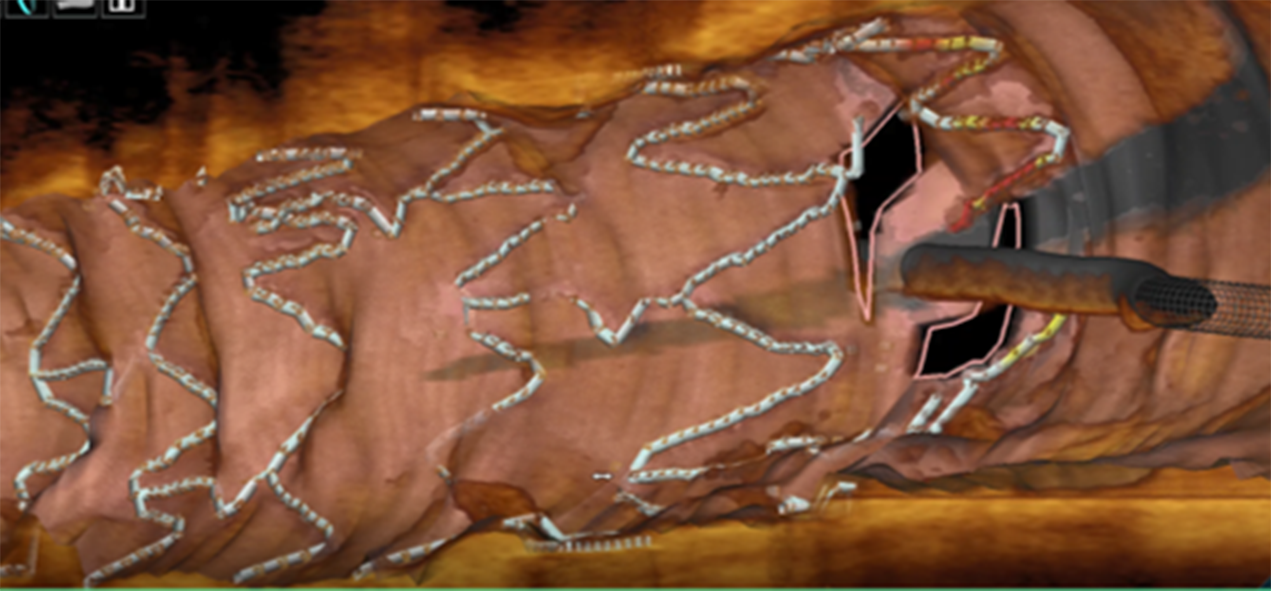
Figure 2a
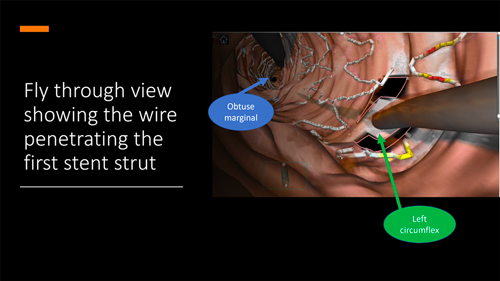
Figure 2b
(4) First step kissing opened the single stent cell and avoided distortion of the stent (Fig3).
Figure 3
(5) Main branch stent was deployed (Fig 4).
Figure 4
(6) Proximal Optimization Technique (POT) was done to open the side branch ostium and facilitate distal-cell side branch wire crossing (Fig 5).
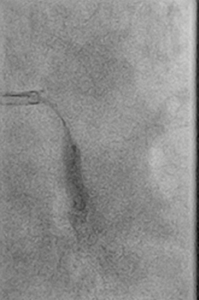
Figure 5
(7) Another workhorse wire was passed into side branch through the distal cell of side branch ostium. (8) Wire position was then confirmed by OCT (Fig 6, Movie 6).
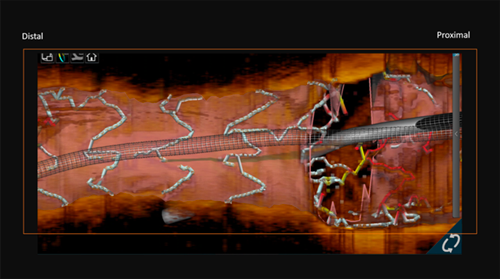
Figure 6
Movie 6
(9) Second Kissing and POT (Fig 7a-b)
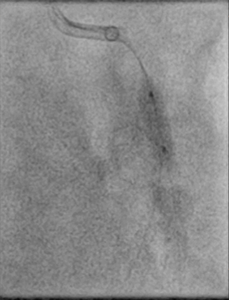
Figure 7a
Figure 7b
OCT was used to assess the result after stenting (Fig 8a-b, movie 8a-c). Final result was satisfactory (Fig 9)
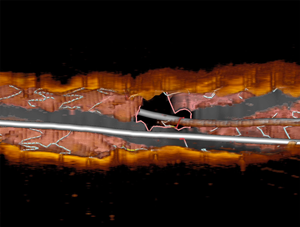
Figure 8a
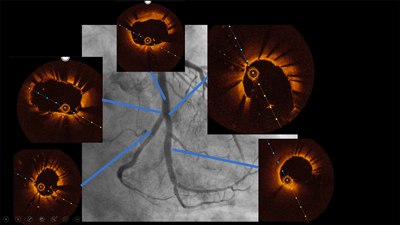
Figure 8b
Movie 8a
Movie 8b
Movie 8c

Figure 9
Why Double Kissing?
Double kissing culotte has a potential advantage of minimizing distortion of stents and reducing acute malapposition. DK mini-culotte was shown to significantly reduce target vessel revascularization/target lesion revascularization and side branch restenosis rate compared with provision T-stenting (3). Therefore, DK-string culotte can be done with minimal overlapping of stent struts without significant distortion of stents.
Special concern and solution:
Although String Culotte technique is a feasible, safe and attractive technique, only small studies with limited sample size were performed. (1-3). On the other hand, there is a potential problem of creating a "napkin effect". It was described to be a potential problem where the side stent cell could not be expanded widely. Therefore, specific side stent cell expansion limit must be taken into consideration when performing single cell DK string culotte technique. For example, if the side stent opening limitation is less than 3.5mm in diameter, such kind of stent should be avoided if the main vessel reference diameter is more than 3.5mm. Nowadays, in the era of new generation DES with modern stent design, the side stent cell expansion limit of 2-link designed stent and certain big size stent, e.g. 3.5-5.0 mm, could be expanded to around 4.5 – 5.0mm in diameter. This can avoid of creating the "napkin effect".
Additionally, if the bifurcation angle between the main branch and side branch is very narrow eg. less than 30-degree, two stent struts may be necessary to protrude out into the main branch to ensure adequate stent coverage at the superior edge of the side branch ostium. Conversely, if the bifurcation ankle is near 90-degree or more, wiring of stent strut would be difficult and side branch stent strut may be protruded at both superior and inferior edge of side branch ostium. Therefore, DK-String culotte technique should be limited to bifurcation lesion with bifurcation ankle with range from 40 to 80 degree.
Conclusion:
Double-kissing single string culotte technique is an attractive novel 2-stent bifurcation technique with minimal stent overlapping, low malapposition rate and low residual obstruction. Clinical studies showed that it safe, and associated with satisfactory clinical outcomes (3). Large clinical scale studies are necessary to compare the outcome with other 2-stent strategies.
Reference:
- Chen, S. L., Sheiban I, Xu, B. et al. Impact of the complexity of bifurcation lesions treated with drug-eluting stents: the DEFINITION study (Definitions and impact of complEx biFurcation lesIons on clinical outcomes after percutaNeous coronary IntervenTIOn using drug-eluting steNts). JACC Cardiovasc Interv 2014;7:1266–76.
- T. Kawasaki, H. Koga, T. Serikawa. Modified culotte stenting technique for bifurcation lesions: the cross-stenting technique J Invasive Cardiol, 22 (2010), pp. 243-246
- Fan, L., Chen, L., Luo, Y. et al. DK mini-culotte stenting in the treatment of true coronary bifurcation lesions: a propensity score matching comparison with T-provisional stenting. Heart Vessels 31, 308–321 (2016). https://doi.org/10.1007/s00380-014-0611-7